
You’ve tried three different creams. Maybe five. The expensive one from the dermatologist’s office, the cult favorite from the pharmacy, the oil everyone swears by on social media. And your stretch marks look exactly the same.
Here’s what nobody tells you upfront: most stretch mark treatments don’t work. Not in the way you hope they will. The research is clear, but the marketing isn’t. This article contains affiliate links. See our affiliate disclosure for details.
Stretch marks are scars. They form when collagen and elastin fibers in the dermis layer rupture under mechanical stress, pregnancy, rapid growth, or hormonal changes. Once those fibers tear, they don’t spontaneously repair themselves. The skin doesn’t forget.
But some interventions do make a measurable difference. Not elimination. Reduction. This review covers what the evidence actually supports, what’s been tested and failed, and what you can realistically expect from treatments that work. Medically reviewed by Dr. Layla Hassan, Trichologist and Dermatology Consultant.
Key Takeaways
• Stretch marks are permanent dermal scars caused by ruptured collagen and elastin fibers; no treatment fully eliminates them • Tretinoin (prescription retinoid) shows the strongest evidence for reducing early, red stretch marks but doesn’t work on mature white marks • Microneedling and fractional laser treatments can improve texture and color in mature stretch marks but require multiple sessions and professional administration • Over-the-counter creams, oils, and butters have minimal to no evidence of effectiveness despite widespread marketing claims • Prevention during pregnancy shows limited success; genetic factors and rate of skin stretching are stronger predictors than topical products
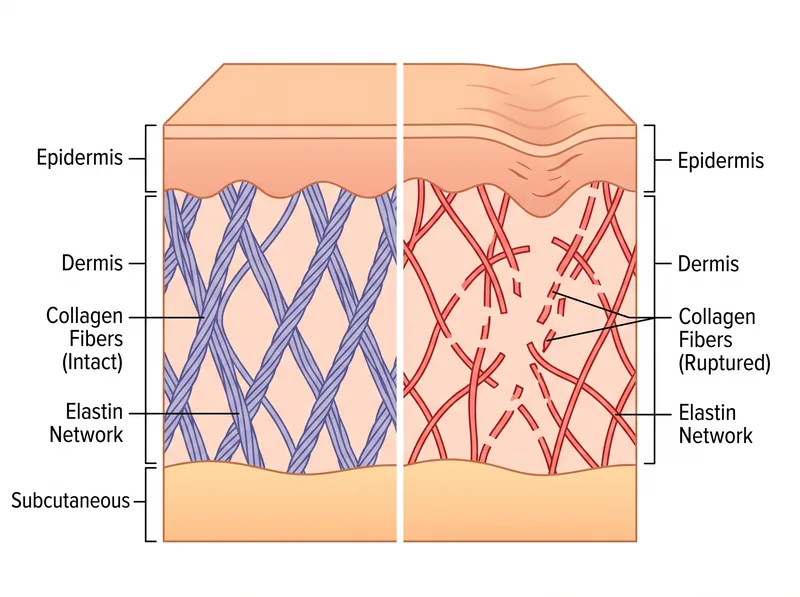 Stretch marks form when collagen and elastin fibers rupture in the dermis layer, creating permanent structural changes that current treatments can’t fully reverse.
Stretch marks form when collagen and elastin fibers rupture in the dermis layer, creating permanent structural changes that current treatments can’t fully reverse.
Why Stretch Marks Form and Why They’re Permanent
Stretch marks, clinically called striae distensae, form in the dermis, the thick middle layer of skin where collagen and elastin provide structural support. When skin stretches faster than these fibers can accommodate, they rupture. The body attempts repair, but the replacement collagen is disorganized and less elastic than the original tissue.
Early stretch marks appear red or purple because blood vessels show through the thinned, damaged dermis. As the marks mature, the blood vessels constrict and the scar tissue becomes pale and atrophic, often appearing silvery-white and slightly depressed below the surrounding skin surface.
This isn’t surface damage. It’s structural. The dermis has been permanently altered. Topical products can’t penetrate deep enough to restructure collagen architecture. This is why creams that work beautifully for surface hyperpigmentation do nothing for stretch marks.
The Gulf climate adds a layer of complication. High heat and humidity increase cortisol, which degrades collagen synthesis. Rapid weight fluctuations from dehydration cycles in extreme heat can exacerbate skin stretching. Hard water reduces skin barrier function, potentially affecting how well any topical treatment penetrates.
What Actually Works: Treatments With Clinical Evidence
Only a handful of interventions have consistent evidence from controlled trials. Here’s what research supports, with realistic expectations.
Tretinoin, a prescription-strength retinoid, is the only topical treatment with solid evidence for reducing early stretch marks. A landmark study in the Archives of Dermatology found that 0.1% tretinoin cream applied nightly for six months reduced the length and width of early striae by 14% and 8% respectively, compared to no improvement in the control group. But it only works on red, recent marks. Once stretch marks turn white, tretinoin shows no benefit.
Tretinoin is also contraindicated during pregnancy and breastfeeding, which eliminates it as an option for the population most likely to develop new stretch marks. And in hot climates, tretinoin increases sun sensitivity significantly, requiring diligent SPF use and often causing irritation that’s harder to manage when you’re already sweating.
Microneedling with a dermaroller or professional dermapen creates controlled micro-injuries that stimulate collagen production. A 2017 systematic review in Dermatologic Surgery found that microneedling improved the appearance of mature stretch marks in 60-70% of patients after four to six sessions, with visible reduction in texture irregularity and some improvement in color. It doesn’t erase the marks, but it makes them less obvious.
Fractional laser treatments, particularly fractional CO2 and erbium lasers, target the dermis with controlled thermal damage to trigger collagen remodeling. Multiple studies show improvement in both texture and pigmentation of mature striae after three to five sessions. A 2017 study in Lasers in Medical Science reported a 25-50% improvement in stretch mark appearance based on physician assessment and patient satisfaction scores.
Both microneedling and laser require professional administration, multiple sessions spaced weeks apart, and realistic expectations. You’re improving texture and blending color, not removing scars. And in the Gulf, post-procedure sun protection is non-negotiable, which means timing treatments during cooler months when you’re not outdoors as much.
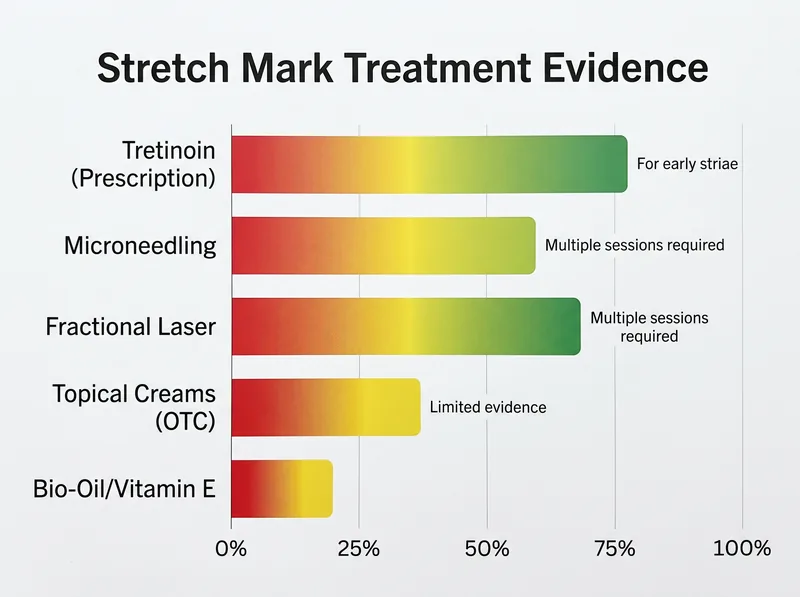 Evidence-based effectiveness ratings for common stretch mark treatments, compiled from systematic reviews and clinical trials.
Evidence-based effectiveness ratings for common stretch mark treatments, compiled from systematic reviews and clinical trials.
What Doesn’t Work: The Evidence Gap in Popular Products
The market for stretch mark creams is enormous. The evidence base is not. Most over-the-counter products marketed for stretch marks have either failed in clinical trials or have never been rigorously tested at all.
Cocoa butter is the classic example. It’s been used for decades, recommended by mothers and midwives, and sold in every pharmacy. But when researchers actually tested it in a randomized controlled trial published in the British Journal of Dermatology, cocoa butter performed no better than placebo. Women who used it daily throughout pregnancy developed stretch marks at the same rate as women who used nothing.
Bio-Oil, another cult favorite, has one small company-funded study showing modest improvement in stretch mark appearance, but independent replication is lacking. A 2018 Cochrane review on interventions for preventing stretch marks during pregnancy found insufficient evidence to recommend any topical preparation, including Bio-Oil, vitamin E oil, olive oil, or various herbal creams.
Centella asiatica (gotu kola) extract shows up in many stretch mark formulations based on preliminary research suggesting it might support collagen synthesis. But the studies are small, often poorly controlled, and the concentration used in commercial products is typically far below what was tested in research settings.
Hyaluronic acid, peptides, and vitamin E are excellent for surface hydration and barrier repair. They do nothing for dermal scarring. Moisturized skin feels better and looks healthier, which is valuable. But it’s not stretch mark reduction. It’s skincare.
Prevention During Pregnancy: What the Research Shows
Preventing stretch marks during pregnancy is the holy grail. The evidence is frustrating. Genetics and the rate of abdominal expansion appear to matter far more than anything you apply topically.
The Cochrane review mentioned earlier analyzed six trials involving over 800 women. None of the topical treatments tested, including cocoa butter, olive oil, and various commercial creams, showed a statistically significant reduction in stretch mark development compared to placebo or no treatment.
One intervention that did show promise: a cream containing Centella asiatica, vitamin E, and collagen-elastin hydrolysates, tested in a study published in the Journal of Obstetrics and Gynaecology. Women who used it twice daily from the first trimester had fewer stretch marks than controls. But the study was small, and the product formulation was specific, not generalizable to other products with similar ingredients listed.
What seems to matter more: gradual, steady weight gain within recommended ranges, adequate hydration, and possibly maintaining skin elasticity through collagen-supporting nutrition. But even women who do everything right still develop stretch marks if their skin can’t keep pace with the rate of stretching.
In the Gulf, pregnancy during summer months may increase risk. Heat stress, dehydration, and cortisol improvion all negatively impact collagen integrity. Staying hydrated and keeping core temperature regulated might matter more than any cream.
Realistic Expectations and What You Can Control
If you have stretch marks, here’s what you can realistically achieve. Early red marks may fade faster with tretinoin if you’re not pregnant and can tolerate retinoids in your climate. Mature white marks can be improved, not erased, with professional microneedling or fractional laser, requiring multiple sessions and ongoing maintenance.
Texture improvement is more achievable than color correction. Depth reduction happens, but slowly. Complete elimination doesn’t. The marks will always be there if you look closely. The goal is making them less noticeable, blending them better with surrounding skin.
Over-the-counter creams won’t hurt, but they won’t deliver the results the packaging implies. If you’re using them for moisture and barrier support, that’s reasonable. If you’re expecting visible stretch mark reduction, you’ll be disappointed. Save your money or redirect it toward treatments with actual evidence.
For skin barrier support in hard water conditions, a chelating body wash like Regrowth+ can help remove mineral buildup that interferes with how well any topical treatment penetrates. It’s not a stretch mark solution, but it’s part of maintaining skin that can actually absorb the products you’re applying.
Acceptance is part of the equation. Stretch marks are common, normal, and not a sign of failure. They’re evidence that your skin stretched, whether from growth, pregnancy, or body changes. The cosmetic industry profits from framing them as a problem requiring endless products. The dermatology evidence says most of those products don’t work.
Professional Treatments: Cost, Commitment, and Outcomes
If you’re considering professional treatment, understand what you’re committing to. Microneedling typically requires four to six sessions spaced four weeks apart, with each session costing between $200-500 depending on the area treated and the provider. Results are gradual and become visible after the second or third session.
Fractional laser treatments are more expensive, ranging from $500-1500 per session, with three to five sessions recommended. Downtime is longer, redness and peeling last several days, and sun protection is critical for weeks afterward. In the Gulf, this means scheduling treatments during winter months when outdoor exposure is lower and UV index isn’t as brutal.
Both treatments work by triggering controlled injury and collagen remodeling. They’re not magic. They’re incremental improvement over months. And they work best on mature, stable stretch marks, not fresh ones still changing color. Patient selection matters. Skin type, mark age, and realistic expectations all influence outcomes.
Some clinics offer combination treatments: microneedling with platelet-rich plasma (PRP), or laser with topical tretinoin post-procedure. The evidence for these combinations is limited and mostly comes from case series, not controlled trials. They may offer additional benefit, but at additional cost and complexity.
References
- Topical tretinoin (retinoic acid) improves early stretch marks - Archives of Dermatology
- Microneedling therapy in atrophic facial scars: an objective assessment - Dermatologic Surgery
- Fractional CO2 laser treatment of striae distensae - Lasers in Medical Science
- The effect of a topically applied cream on striae gravidarum - British Journal of Dermatology
- Interventions for preventing stretch marks in pregnancy - Cochrane Database of Systematic Reviews