
If you’ve got persistent tiny bumps on your upper arms that won’t go away no matter how much you exfoliate, you’re not dealing with acne or clogged pores. You’ve got keratosis pilaris, a harmless but frustrating skin condition that affects nearly 40% of adults and shows up even more aggressively in hot, humid climates.
The bumps feel rough, look like permanent goosebumps, and get worse in summer when you’d most like to wear sleeveless tops. Scrubbing harder doesn’t help. Most moisturisers don’t touch it. And the standard advice about gentle exfoliation often makes things worse in Gulf conditions where heat, sweat, and hard water create a perfect storm for keratin buildup.
Here’s what’s actually happening to your skin, why hot climates make it worse, and the treatment approach that works when you’re dealing with both environmental stress and a genetic tendency toward keratin overproduction. Medically reviewed by Dr. Layla Hassan, Trichologist.
Key Takeaways
• Keratosis pilaris (KP) is caused by excess keratin protein blocking hair follicles, creating rough bumps on arms, thighs, and sometimes face
• Heat, humidity, and sweat make KP worse by increasing inflammation and trapping more keratin in follicles
• Physical scrubs and harsh exfoliation damage the skin barrier without addressing the keratin plugs underneath
• Chemical exfoliants (AHAs like lactic acid and glycolic acid) dissolve keratin buildup more effectively than mechanical scrubbing
• Treatment requires consistent barrier repair alongside exfoliation, especially in climates with hard water and extreme heat
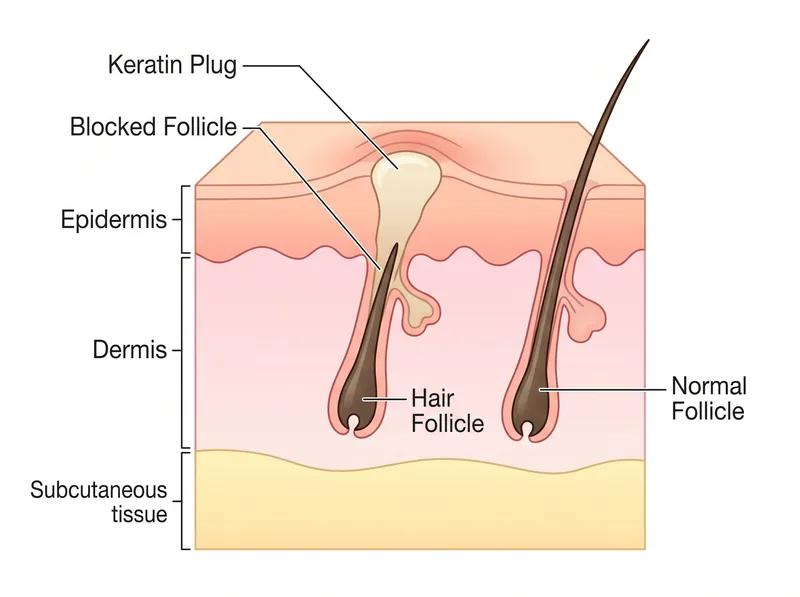 Keratosis pilaris occurs when excess keratin blocks the hair follicle opening, creating the characteristic bump
Keratosis pilaris occurs when excess keratin blocks the hair follicle opening, creating the characteristic bump
What Keratosis Pilaris Actually Is
Keratosis pilaris happens when your skin produces too much keratin, the structural protein that makes up your outer skin layer, hair, and nails. That excess keratin doesn’t shed properly. Instead, it builds up around hair follicles and blocks the follicle opening.
The result is those characteristic small, rough bumps. They’re not inflamed (usually). They’re not infected. They’re just plugged follicles with a keratin cap sitting on top.
KP most commonly appears on the outer upper arms, front thighs, buttocks, and sometimes cheeks. The bumps are typically flesh-colored or slightly red, and the surrounding skin often feels rough like sandpaper even where individual bumps aren’t visible.
It’s genetic. If one parent has it, you’ve got about a 50% chance of developing it. If both parents have it, your odds jump to around 75%. The condition usually appears in childhood, improves slightly in adolescence, then returns or persists into adulthood for many people.
Why Hot Climates Make KP Worse
Heat and humidity create a cascade of problems for keratosis pilaris. First, you’re sweating more. That sweat sits on the skin surface, mixes with dead skin cells and sebum, and creates an environment where keratin plugs form more readily.
Second, heat increases skin inflammation generally. Research shows that improved skin temperature triggers inflammatory mediators that make existing KP bumps redder and more noticeable. In Gulf summers, your baseline skin temperature is higher for hours every day.
Third, the combination of outdoor heat and indoor air conditioning creates dramatic humidity swings. Your skin barrier struggles to adapt, leading to increased transepidermal water loss and a compromised barrier that can’t regulate keratin production properly.
Hard water makes everything worse. The mineral content in Gulf water supplies leaves a film on skin that interferes with proper cell turnover. You’re essentially layering mineral deposits on top of keratin plugs, making the texture even rougher and preventing topical treatments from penetrating effectively.
 Chemical exfoliants like AHAs work better than physical scrubs for dissolving the keratin plugs in KP
Chemical exfoliants like AHAs work better than physical scrubs for dissolving the keratin plugs in KP
Why Standard Exfoliation Advice Fails Here
Most dermatology resources recommend gentle physical exfoliation for KP. That advice assumes you’re living in a temperate climate with soft water and moderate humidity. It doesn’t account for what happens when you’re exfoliating skin that’s already stressed from heat exposure and mineral buildup.
Physical scrubs (sugar scrubs, salt scrubs, exfoliating gloves) remove surface dead skin cells, but they don’t dissolve the keratin plugs inside the follicles. You’re buffing the top layer while the actual problem sits underneath, untouched.
Worse, aggressive scrubbing damages the skin barrier. In hot climates where your barrier is already compromised from UV exposure and environmental stress, that damage compounds. Your skin responds by producing more keratin as a protective response, making the KP worse over time.
The scrub-moisturise cycle most people fall into creates a temporary improvement (the surface feels smoother) followed by a rebound effect where the bumps return within days, often more pronounced than before.
The Chemical Exfoliation Approach That Actually Works
Alpha hydroxy acids (AHAs) are the most effective treatment for keratosis pilaris because they work on the keratin plugs themselves, not just the surface skin. Lactic acid and glycolic acid dissolve the bonds holding dead skin cells together and help clear the keratin buildup from follicle openings.
A 2005 study in the Journal of Cosmetic Dermatology found that 12% lactic acid lotion applied twice daily reduced KP bumps by 56% after four weeks, with continued improvement over 12 weeks. The key was consistent use, not aggressive application.
For hot climates, you want a formulation that’s hydrating alongside exfoliating. Lactic acid is hygroscopic, meaning it draws moisture into the skin while it works. That’s critical when you’re dealing with both keratin buildup and barrier dehydration from heat exposure.
Start with a 10-12% AHA lotion applied once daily after showering. The skin is slightly damp, which helps the product penetrate without causing irritation. You’re not scrubbing it in. You’re smoothing it on and letting the chemistry do the work.
If you’re using a chelating shampoo like Regrowth+ to address hard water buildup on your scalp, the same principle applies to body skin. Chemical treatment works better than mechanical scrubbing when you’re dealing with mineral and keratin deposits that physical exfoliation can’t reach.
Barrier Repair Is Non-Negotiable
You can’t exfoliate your way out of KP if your skin barrier is compromised. The two have to happen together. Chemical exfoliation removes the keratin plugs, but barrier repair prevents new ones from forming as aggressively.
Look for body moisturisers with ceramides, cholesterol, and fatty acids in a 3:1:1 ratio. That’s the lipid composition your skin barrier needs to function properly. Ceramides for Skin Barrier Repair in Dry Climates covers why this ratio matters and how to identify it in product formulations.
Urea is particularly effective for KP because it’s both a humectant (draws water into skin) and a keratolytic (helps break down keratin). A 10-20% urea cream applied after your AHA treatment creates a one-two punch: the AHA dissolves plugs, the urea keeps them from reforming while maintaining hydration.
In hot climates, you need barrier repair that can handle sweat. Lightweight gel-creams with hyaluronic acid and niacinamide work better than heavy occlusives that trap heat and sweat against the skin. Niacinamide for Skin in Humidity explains why this ingredient is particularly effective in Gulf conditions.
The Treatment Protocol That Works in Gulf Heat
Morning routine: Shower with lukewarm water (hot water strips the barrier further). Pat skin dry, leaving it slightly damp. Apply a lightweight barrier repair moisturiser with ceramides and niacinamide. Wait 10 minutes before getting dressed to avoid product transfer and allow absorption.
Evening routine: Shower to remove sweat and environmental buildup. Pat dry. Apply your AHA lotion (10-12% lactic acid or glycolic acid) to affected areas. Wait 5-10 minutes for absorption. Follow with a urea-based moisturiser (10-20% concentration). This is your active treatment window.
Twice weekly: Use a gentle, non-foaming cleanser in the shower instead of soap. Soap strips natural oils and changes the pH balance your skin needs to regulate keratin production. On these days, skip the evening AHA and just use barrier repair moisturiser.
Weekly maintenance: After your regular evening routine, apply a thick occlusive (like petroleum jelly or a heavy balm) over the urea moisturiser on affected areas. This is particularly important if you’ve been in chlorinated pools or had extended sun exposure that week.
You’ll see initial improvement in texture within 2-3 weeks. The bumps start to flatten and the roughness decreases. Full improvement takes 8-12 weeks of consistent treatment. Miss three days in a row and you’ll likely see some regression, especially during summer months.
What Makes KP Worse Beyond Climate
Hormonal fluctuations affect keratin production. Many women notice their KP worsens during pregnancy, postpartum, or perimenopause. Perimenopause Hair Thinning discusses how declining estrogen affects keratin regulation, and the same mechanism impacts skin keratin production.
Vitamin A deficiency is associated with keratosis pilaris. Your skin needs retinoids to regulate keratin production and cell turnover. If you’re low in vitamin A, your body overproduces keratin as a compensatory mechanism. The American Academy of Dermatology notes that topical retinoids can help KP, but dietary vitamin A is the foundation.
Thyroid dysfunction often shows up as worsening KP. Both hypothyroidism and hyperthyroidism can change keratin metabolism. If your KP suddenly gets significantly worse without an obvious environmental trigger, it’s worth checking thyroid function. Thyroid and Hair Loss in Women covers the full range of thyroid-related skin and hair changes.
Chronic inflammation from any source (poor diet, stress, lack of sleep) makes KP more pronounced. Your skin responds to systemic inflammation by increasing keratin production as a protective mechanism. Managing overall inflammation often leads to noticeable improvement in KP severity.
When to See a Dermatologist
If over-the-counter AHA treatments don’t produce noticeable improvement after 12 weeks of consistent use, prescription options exist. Topical retinoids (tretinoin, adapalene) are more potent keratolytics than AHAs and may work when other treatments fail.
Prescription-strength urea (20-40%) or salicylic acid (6%) formulations can be compounded for severe cases. These require medical supervision because they’re strong enough to cause significant irritation if used incorrectly, especially in hot climates where skin is already stressed.
Laser treatments (pulsed dye laser, intense pulsed light) can reduce the redness associated with KP and may help with the bumps themselves by targeting the inflammation around follicles. This is typically reserved for cases where the cosmetic impact is significant and topical treatments haven’t worked.
If your KP is accompanied by other skin symptoms (severe itching, weeping, widespread inflammation), you may have a different condition that requires medical diagnosis. Eczema, folliculitis, and other inflammatory skin conditions can coexist with or mimic KP.
References
- Heat Stress and Inflammatory Skin Responses - PMC - National Center for Biotechnology Information
- Efficacy of Lactic Acid in the Treatment of Keratosis Pilaris - PubMed - Journal of Cosmetic Dermatology
- Keratosis Pilaris: Diagnosis and Treatment - American Academy of Dermatology
- Skin Barrier Function and Keratin Disorders - PubMed Central