
If you’ve ever stood in front of a mirror in changing room lighting and thought ‘when did that happen,’ you’re not alone. Cellulite appears on roughly 90% of women at some point after puberty. It’s not a flaw. It’s not a sign you’re doing something wrong. It’s a structural characteristic of how female bodies store fat and how connective tissue is organized under the skin.
But that hasn’t stopped the beauty industry from building a billion-dollar market around making you feel like it’s a problem you need to fix. The Gulf climate adds another layer to this: heat, hard water, and indoor air conditioning can all affect skin texture and hydration, which influences how visible cellulite appears. This article contains affiliate links. See our affiliate disclosure for details.
Here’s what actually causes cellulite, what the research says about treatments that work, and how to distinguish between evidence-based interventions and expensive marketing. Medically reviewed by Dr. Layla Hassan, Trichologist.
What Cellulite Actually Is (And Why Women Get It More)
Cellulite is the dimpled appearance that occurs when subcutaneous fat pushes against fibrous connective tissue bands (called septae) that tether the skin to deeper structures. The fat cells bulge upward between these bands, creating the characteristic dimpled or ‘orange peel’ texture on the skin surface.
Women develop cellulite more frequently than men because of structural differences in how connective tissue is arranged. In women, the septae run vertically, like parallel columns. This allows fat to push through more easily. In men, the septae cross-hatch diagonally, creating a net-like structure that holds fat more evenly. Women also have thinner skin on average, which makes the underlying structure more visible.
Estrogen plays a role too. Research published in the Journal of Cosmetic and Laser Therapy shows that estrogen influences fat distribution, connective tissue structure, and microcirculation in the skin. This is why cellulite often appears or worsens during puberty, pregnancy, and perimenopause, when estrogen levels fluctuate.
It’s not about being overweight. Thin women get cellulite. Athletes get cellulite. It’s a secondary sex characteristic, like breasts or wider hips. The difference is that no one’s trying to sell you a cream to fix those.
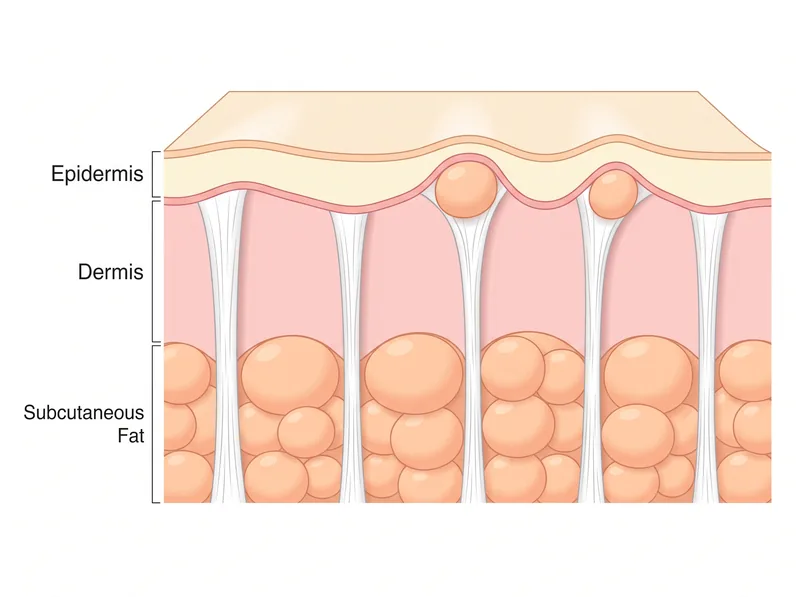 How cellulite forms: fat cells push against fibrous connective tissue bands, creating the dimpled appearance on the skin surface.
How cellulite forms: fat cells push against fibrous connective tissue bands, creating the dimpled appearance on the skin surface.
What Causes Cellulite to Appear or Worsen
Genetics is the biggest factor. If your mother has cellulite, you’re more likely to develop it. A review in the Journal of the European Academy of Dermatology found that genetic factors influence skin thickness, connective tissue architecture, fat distribution, and circulation patterns, all of which affect cellulite visibility.
Age matters because skin loses collagen and elasticity over time. Thinner, less elastic skin shows the underlying fat structure more clearly. Muscle tone also declines with age, which reduces the smoothing effect that toned muscle provides under the skin. This doesn’t mean cellulite is inevitable with aging, but it does mean the factors that make it visible increase.
Body fat percentage influences how much fat is available to push against the septae. But it’s not linear. You can lose weight and still have cellulite because the structural arrangement of connective tissue doesn’t change. Some women notice cellulite becomes more visible when they lose muscle mass, even if they lose fat, because muscle provides a firmer base under the skin.
Hormonal shifts during pregnancy, menopause, or when starting or stopping hormonal contraception can trigger changes in fat distribution and fluid retention. Estrogen decline during menopause specifically affects collagen production and skin thickness, both of which influence how cellulite appears.
Lifestyle factors like poor circulation, dehydration, and prolonged sitting can worsen the appearance of cellulite. In the Gulf, where indoor air conditioning runs constantly and desalinated water affects hydration, skin can become dehydrated more easily, making texture more pronounced. This doesn’t cause cellulite, but it can make existing cellulite more visible.
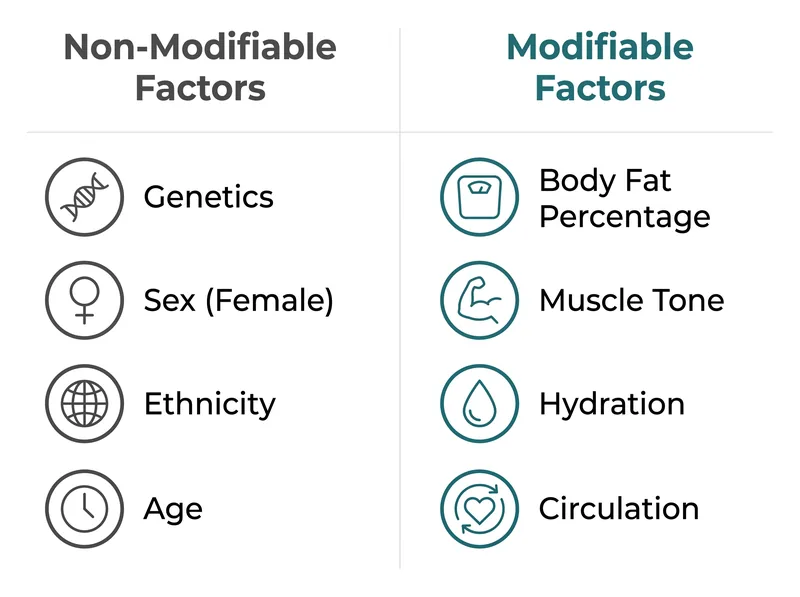 Risk factors you can and can’t control: genetics, hormones, age, and lifestyle all play a role.
Risk factors you can and can’t control: genetics, hormones, age, and lifestyle all play a role.
Treatments That Have Clinical Evidence
Let’s start with what actually works, according to peer-reviewed research. These aren’t cheap, and none of them are permanent, but they do produce measurable changes in cellulite appearance.
Subcision is a minor surgical procedure where a dermatologist or plastic surgeon inserts a small blade under the skin to cut the fibrous septae that create the dimpling. A study in Dermatologic Surgery found that subcision improved cellulite appearance by an average of 2 grades on a 4-point severity scale, with results lasting up to two years. It’s invasive, it requires local anesthesia, and it costs several thousand dollars. But it addresses the structural cause.
Acoustic wave therapy (also called shockwave therapy) uses high-energy sound waves to break down fibrous tissue and stimulate collagen production. Research in the Journal of Cosmetic and Laser Therapy showed that patients who received 6-12 sessions saw a 15-25% reduction in cellulite severity scores. Results are temporary, lasting 6-12 months, and require maintenance sessions.
Radiofrequency and laser treatments heat the deeper layers of skin to stimulate collagen remodeling and reduce fat cell size. A review in Clinical, Cosmetic and Investigational Dermatology found that combination treatments using radiofrequency plus massage or suction showed moderate improvement in cellulite appearance. Results vary significantly between individuals, and multiple sessions are required.
These treatments work through different mechanisms, but they all address the structural components of cellulite: the fibrous bands, the fat distribution, or the skin thickness. They’re not magic, and they’re not permanent, but they’re backed by controlled studies showing measurable changes.
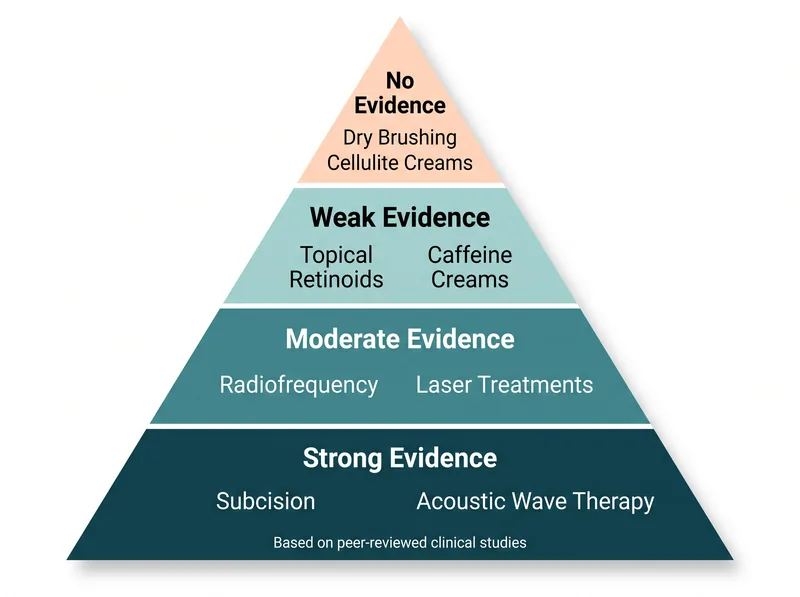 Treatment efficacy hierarchy: what the research actually supports versus what’s marketed most aggressively.
Treatment efficacy hierarchy: what the research actually supports versus what’s marketed most aggressively.
Topical Treatments: What the Evidence Actually Shows
Topical retinoids (prescription-strength tretinoin or over-the-counter retinol) can thicken the skin over time, which may reduce the visibility of cellulite. A study published in the European Journal of Dermatology found that 0.3% retinol applied twice daily for six months produced a slight improvement in cellulite appearance, likely due to increased collagen production and skin thickening. The effect is modest, and it requires consistent long-term use.
Caffeine creams are marketed heavily for cellulite, and there’s some mechanistic logic: caffeine is a vasoconstrictor and may temporarily dehydrate fat cells, making them appear smaller. But the evidence is weak. A review in the Journal of Cosmetic Dermatology concluded that while caffeine can penetrate the skin, there’s insufficient evidence that topical application produces clinically significant or lasting changes in cellulite appearance.
Most cellulite creams contain a mix of caffeine, retinol, peptides, and botanical extracts. They’re not harmful (unless you have sensitive skin), but they’re not going to deliver the dramatic before-and-after photos you see in ads. Those photos are usually taken under different lighting, with different postures, or immediately after massage, which temporarily improves fluid distribution.
If you’re going to use a topical product, retinol is your best bet, but manage your expectations. You’re looking at marginal improvement over six months, not transformation.
Lifestyle Interventions That Help (And Why)
Strength training won’t eliminate cellulite, but it can reduce its appearance by building muscle under the skin, which creates a firmer, smoother surface. Research in the Journal of Sports Science and Medicine found that women who completed a 12-week lower-body resistance training program showed a reduction in thigh circumference and a modest improvement in cellulite severity scores.
The key is building muscle in the areas where cellulite appears, typically the glutes, hamstrings, and quadriceps. Squats, lunges, deadlifts, and hip thrusts are the movements that matter. Cardio alone won’t do it because it doesn’t build the muscle mass needed to change the underlying structure.
Hydration affects skin plumpness and texture. Dehydrated skin looks thinner and more crepey, which makes cellulite more visible. In the Gulf, where heat and indoor air conditioning both pull moisture from your skin, staying hydrated is harder than it sounds. You need more water than you think, and you need to lock it in with a good body moisturizer.
Dry brushing, massage, and foam rolling are often marketed as cellulite treatments. They don’t change the structure of fat or connective tissue, but they do temporarily improve circulation and lymphatic drainage, which can reduce fluid retention and make skin look smoother for a few hours. It’s not a treatment. It’s a temporary cosmetic effect. If it feels good and you enjoy the ritual, fine. But don’t expect lasting changes.
Maintaining a stable weight helps because rapid weight gain or loss can stretch the skin and connective tissue, potentially worsening the appearance of cellulite. This isn’t about being thin. It’s about avoiding the yo-yo cycle that stresses the skin’s structural integrity.
What Doesn’t Work (Despite the Marketing)
Cellulite creams that promise to ‘melt fat’ or ‘break down cellulite’ are lying. Topical products cannot penetrate deeply enough to affect subcutaneous fat. Even if they could, fat cells don’t just dissolve because you rubbed caffeine on them. The FDA does not recognize any topical product as effective for cellulite reduction.
Detox teas, supplements, and cleanses marketed for cellulite are nonsense. Cellulite is not caused by ‘toxins’ or poor digestion. It’s a structural characteristic of how fat and connective tissue are arranged. No amount of lemon water or activated charcoal will change that.
Body wraps and spa treatments that claim to reduce cellulite work through temporary dehydration. You might lose an inch of circumference immediately after because you’ve sweated out water. You’ll gain it back as soon as you rehydrate. It’s a short-term cosmetic trick, not a treatment.
Cupping therapy is sometimes promoted for cellulite reduction. There’s no evidence it works. It may cause temporary inflammation and increased blood flow, which could make the skin look temporarily smoother, but it doesn’t address the fibrous bands or fat distribution that cause cellulite.
Cellulite leggings, compression garments, and anti-cellulite underwear compress the skin, which may temporarily smooth the appearance. But the moment you take them off, you’re back to baseline. They’re shapewear, not treatment.
Environmental Factors in the Gulf That Affect Skin Texture
The Gulf climate creates a specific set of challenges for skin texture and hydration. Extreme heat and sun exposure break down collagen and elastin, which are the structural proteins that keep skin firm and smooth. Over time, this makes cellulite more visible because the skin becomes thinner and less resilient.
Indoor air conditioning runs year-round in the region, and it strips moisture from the air and from your skin. Prolonged exposure to dry indoor air dehydrates the skin’s outer layers, making texture more pronounced. If your skin feels tight or looks crepey, that’s a hydration issue, not a cellulite issue, but the two overlap visually.
Hard water in the Gulf contains high levels of calcium and magnesium, which can leave a residue on the skin that changes the moisture barrier. This doesn’t cause cellulite, but it can make skin feel rough and look dull, which draws more attention to texture irregularities. Using a chelating body wash (like Regrowth+ for your scalp) can help remove mineral buildup and restore smoother skin texture.
Sun damage is cumulative. If you’re spending time outdoors or by the pool without adequate sun protection, you’re accelerating collagen breakdown. Broad-spectrum sunscreen isn’t just for preventing skin cancer. It’s also for preserving the structural integrity of your skin.
What You Can Realistically Expect From Any Treatment
No treatment eliminates cellulite permanently. Even surgical interventions like subcision require repeat sessions over time because the body continues to produce connective tissue and store fat. The goal is reduction in visibility, not elimination.
Results are highly individual. Two women with similar body types and cellulite severity can undergo the same treatment and see different outcomes. Genetics, skin thickness, fat distribution, and how your body responds to collagen stimulation all play a role. This is why before-and-after photos in marketing materials are misleading. They show the best-case scenario, not the average result.
Maintenance is required for all treatments. Whether it’s continuing to apply retinol, scheduling follow-up radiofrequency sessions, or maintaining muscle mass through strength training, cellulite reduction is not a one-and-done intervention. It’s ongoing management.
The most effective approach is combination therapy. Research in Aesthetic Surgery Journal found that patients who combined treatments (such as subcision plus radiofrequency, or acoustic wave therapy plus topical retinoids) saw better results than those who used a single modality. But combination therapy also means higher cost and more time commitment.
If you’re considering professional treatment, consult a board-certified dermatologist or plastic surgeon who specializes in body contouring. Avoid medspas or clinics that use high-pressure sales tactics or promise unrealistic results. Ask to see before-and-after photos of real patients (not stock images), and ask about the number of sessions required and the expected duration of results.
References
- Cellulite: A Review of Its Physiology and Treatment - Journal of Cosmetic and Laser Therapy
- Cellulite: Pathophysiology and Treatment - Journal of the European Academy of Dermatology and Venereology
- Subcision for Cellulite: Clinical Improvement After a Single Treatment - Dermatologic Surgery
- Acoustic Wave Therapy for Cellulite Treatment - Journal of Cosmetic and Laser Therapy
- Noninvasive Treatments for Cellulite: A Complete Review - Clinical, Cosmetic and Investigational Dermatology
- Topical Retinol Improves Cellulite - European Journal of Dermatology
- Caffeine and Its Effects on the Skin - Journal of Cosmetic Dermatology
- Effects of Resistance Training on Cellulite - Journal of Sports Science and Medicine