
You’ve noticed your ponytail is thinner. Your part seems wider. You can see more scalp when you pull your hair back. And when you mention it to your doctor, the response is vague: stress, maybe, or just getting older. But you’re 32. This doesn’t feel like aging.
If you have PCOS, your hair loss likely follows a specific pattern that most women and many doctors don’t recognise. It’s not the all-over shedding of telogen effluvium. It’s androgenic alopecia, the same mechanism behind male pattern baldness, and it affects up to 40% of women with polycystic ovary syndrome. The thinning concentrates at your crown. Your temples may recede slightly. Your frontal hairline often stays intact.
This article contains affiliate links. See our affiliate disclosure for details.
The challenge in hot, hard water climates is that environmental damage masks the hormonal pattern. Mineral buildup creates a separate layer of hair texture changes that can delay diagnosis by months or years. Here’s what PCOS does to your hair, how the androgen pattern differs from other types of loss, and why clinical workup matters even when environmental factors are clearly present. Medically reviewed by Dr. Layla Hassan, Trichologist.
Key Takeaways
• PCOS hair loss follows an androgenic pattern: crown thinning with frontal hairline preservation, often with temple recession, distinct from diffuse shedding.
• Improved androgens (testosterone and DHT) progressively miniaturize hair follicles, shortening growth phase and producing finer, shorter hairs over time.
• Environmental factors like hard water create a separate layer of damage that can mask the hormonal pattern and delay diagnosis.
• Clinical workup is essential: hormone panels, ferritin levels, thyroid function, and scalp examination differentiate PCOS hair loss from other causes.
• Treatment requires addressing both the hormonal cause (often spironolactone or birth control) and environmental damage (chelating shampoos, protective routines).
 PCOS-related hair loss follows a distinct androgenic pattern: crown thinning with frontal preservation, often with temple recession.
PCOS-related hair loss follows a distinct androgenic pattern: crown thinning with frontal preservation, often with temple recession.
The Androgenic Pattern: What PCOS Hair Loss Actually Looks Like
Female pattern hair loss from PCOS doesn’t look like male pattern baldness, but it follows the same hormonal mechanism. You won’t see a receding hairline in the classic M-shape. Instead, the thinning concentrates at your crown and vertex, the area at the top and back of your head where you’d naturally part your hair.
Your frontal hairline typically stays intact. That’s the key differentiator. When you look in the mirror face-on, your hairline looks normal. But when you see the top of your head in photos or pull your hair into a ponytail, the thinning is obvious. The part widens. You see scalp. The hair at your crown looks noticeably sparser than the hair framing your face.
Some women also develop slight temple recession, the areas just above your ears where your hairline curves back. Research published in Dermatology and Therapy found that 67% of women with PCOS-related hair loss showed this combined crown-and-temple pattern, compared to just 12% of women with non-androgenic diffuse thinning.
The progression is gradual. You don’t wake up one day with visible scalp. Instead, over months to years, the hair in the affected areas becomes finer, shorter, and less pigmented. The follicles miniaturize, producing vellus hairs (the soft, nearly invisible hairs that cover most of your body) instead of terminal hairs (the thick, pigmented strands you’re used to). Eventually, some follicles stop producing visible hair entirely.
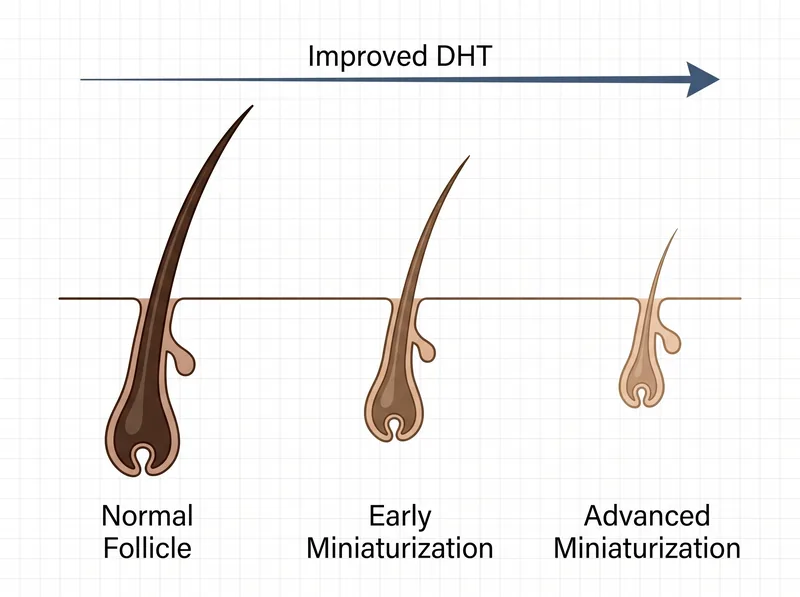 Improved DHT from PCOS progressively shrinks follicles, shortening growth phase and producing finer, shorter hairs.
Improved DHT from PCOS progressively shrinks follicles, shortening growth phase and producing finer, shorter hairs.
How Androgens Damage Hair Follicles in PCOS
PCOS causes improved androgens, primarily testosterone and its more potent metabolite, dihydrotestosterone (DHT). In genetically susceptible hair follicles, particularly those at the crown and temples, DHT binds to androgen receptors and triggers a cascade that shortens the growth phase of the hair cycle.
Normal hair grows for 2-7 years before entering a resting phase and eventually shedding. DHT-affected follicles compress that growth phase down to months. The hair doesn’t have time to grow long or thick. It emerges, reaches a few inches, and sheds. With each cycle, the follicle shrinks further. The hair becomes finer. The color fades. The density decreases.
This process is called miniaturization, and it’s progressive. A 2020 study in the Journal of Clinical Endocrinology & Metabolism tracked 156 women with PCOS over five years and found that untreated androgenic alopecia worsened in 73% of participants, with an average 18% decrease in hair density at the crown.
The genetic susceptibility matters. Not all women with improved androgens lose hair. The follicles at your crown and temples need to have androgen receptors that are particularly sensitive to DHT. That’s why some women with severe PCOS and very high testosterone levels maintain full hair, while others with only mildly improved androgens develop significant thinning. It’s the follicle’s response to the hormone, not just the hormone level itself.
Environmental Damage Masks the Hormonal Pattern
In regions with hard water and extreme heat, environmental damage creates a confounding layer. Mineral buildup from calcium and magnesium coats the hair shaft, making all your hair feel coarse, dry, and brittle. UV exposure degrades the protein structure. Low humidity strips moisture. The result is hair that looks and feels damaged everywhere, not just at the crown.
This diffuse environmental damage can obscure the androgenic pattern. When all your hair feels terrible, it’s harder to notice that the crown is thinning more than the rest. You attribute the texture change to the water, the heat, the move. You try different products. You deep condition. You avoid heat styling. And the thinning continues underneath, undiagnosed.
The timeline compounds the confusion. PCOS hair loss is gradual. Environmental damage is immediate. You move to a hot, hard water climate, and within weeks, your hair feels different. You assume that’s the problem. But six months later, your ponytail is noticeably thinner. A year later, you can see scalp at your crown. By the time you realise it’s not just environmental, the androgenic pattern is well-established.
That’s why clinical workup matters even when environmental factors are obvious. A chelating shampoo like Regrowth+ removes the mineral coating and restores your hair’s natural texture, which makes the underlying thinning pattern visible. If the crown is significantly sparser than the sides and front even after you’ve addressed the hard water damage, that’s a hormonal issue that needs medical evaluation.
Clinical Workup: What Testing Actually Reveals
Diagnosing PCOS-related hair loss requires hormone panels, not just visual assessment. Your doctor should test total and free testosterone, DHEA-S, androstenedione, and sex hormone-binding globulin (SHBG). In PCOS, you’ll typically see improved free testosterone (the biologically active form) even if total testosterone is normal, because SHBG is often low.
But androgens aren’t the only factor. Ferritin (stored iron) below 40 ng/mL exacerbates hair loss even when hemoglobin is normal. Thyroid dysfunction, particularly subclinical hypothyroidism, mimics androgenic alopecia. Vitamin D deficiency, common in women who cover their skin in sunny climates, affects follicle cycling. Iron deficiency alone can cause diffuse thinning that looks similar to the PCOS pattern.
A complete panel should include: TSH, free T3, free T4, ferritin, vitamin D, fasting insulin, and a full androgen profile. Some endocrinologists also check anti-Müllerian hormone (AMH) and do a pelvic ultrasound to confirm polycystic ovaries, though hair loss can occur with PCOS even without visible cysts.
Scalp examination by a dermatologist or trichologist adds diagnostic clarity. They’ll look at hair density, miniaturization patterns, and scalp health. A pull test (gently tugging 50-60 hairs to see how many shed) differentiates active shedding from chronic thinning. Dermoscopy, a magnified view of the scalp, reveals follicular units and miniaturized hairs that aren’t visible to the naked eye. This clinical assessment, combined with labs, confirms whether you’re dealing with androgenic alopecia, telogen effluvium, or both.
Treatment Requires Addressing Both Layers
PCOS hair loss doesn’t respond to environmental fixes alone. You can remove every trace of mineral buildup, optimise your water, use the gentlest products, and the androgenic thinning will continue. That’s because the problem is internal. The follicles are responding to circulating DHT. Until you lower androgen levels or block their effect on the follicle, the miniaturization progresses.
The most common medical treatments are spironolactone (an androgen blocker) and combined oral contraceptives (which increase SHBG and lower free testosterone). The American Academy of Dermatology recommends spironolactone as first-line therapy for female pattern hair loss, typically starting at 100-150 mg daily. Results take 6-12 months. You won’t see new growth immediately. Instead, the thinning stabilizes, then very gradually improves.
Minoxidil (topical or oral) is often added. It doesn’t address the androgen issue, but it prolongs the growth phase and can thicken existing miniaturized hairs. The 5% foam formulation works better than the 2% solution for women. Consistency matters. Missing applications reduces effectiveness.
But here’s what medical treatment doesn’t fix: the environmental damage. Your hair may stop thinning, but if it’s still coated in minerals, dried out by low humidity, and damaged by UV exposure, it won’t look or feel healthy. That’s where the protective routine comes in. Chelating shampoos remove buildup. Leave-in conditioners with humectants retain moisture. UV protectants shield the hair shaft. Satin pillowcases reduce friction. You’re treating two separate problems: the hormonal cause of the thinning and the environmental factors that degrade the hair you still have.
What Improvement Actually Looks Like
Realistic expectations matter. PCOS hair loss treatment doesn’t restore your 18-year-old hair density. It stabilizes the thinning and, over time, produces modest regrowth. A 2017 meta-analysis in Dermatologic Therapy found that women using combined spironolactone and minoxidil saw an average 12-15% increase in hair density at the crown after 12 months, with 64% reporting subjective improvement.
The first sign of response is usually decreased shedding. You notice less hair in the shower drain, on your pillow, in your brush. That happens around month 3-4. Visible regrowth takes longer, often 6-9 months. And it’s subtle. You might see fine baby hairs at the hairline or increased density at the part. Your ponytail feels slightly thicker. Photos show less visible scalp.
The environmental improvements are faster. Remove mineral buildup with a chelating treatment, and within one wash, your hair feels softer, lighter, more manageable. Add a hydrating routine, and the texture improves within weeks. That immediate environmental response can create false hope that the thinning itself will reverse quickly. It won’t. The hormonal regrowth is slow. But the combination of both treatments, the medical intervention for the follicles and the protective routine for the hair shaft, produces the best cosmetic outcome.
Maintenance is lifelong. PCOS is a chronic condition. If you stop the androgen-blocking medication, the thinning resumes. If you move back to a soft water climate and abandon the chelating routine, you won’t need it anymore. But as long as you’re living with both the hormonal condition and the environmental stressors, you’re managing both.
References
- Female Pattern Hair Loss and Its Relationship with Permanent Oxidative Hair Dye Use and Other Risk Factors - PubMed Central
- Prevalence of Female Pattern Hair Loss in Premenopausal Women: A Systematic Review and Meta-analysis - PubMed
- Hair Loss: Female Pattern Baldness - American Academy of Dermatology
- Efficacy of Spironolactone in Female Pattern Hair Loss: A Systematic Review and Meta-analysis - PubMed